Direct Pulp Capping (Partial Coronal Pulpectomy)
Member Only Content
Members Links
Printer Articles
- Anatomy
- Dental Extractions of Single Rooted Teeth
- Direct Pulp Capping (Partial Coronal Pulpectomy)
- Extractions
- Feline Dental Radiography
- Homecare
- Infra-orbital nerve block in the dog.
- Introduction to Anaesthesia
- Members Lectures
- Paedodontics
- Periodontal Disease 3 – Saving the Periodontally Diseased Tooth
- Periodontology
- Pocket Pets and Exotics
- Procedure Videos
- Reference Manuals
- Rest acid etch
- Restoratives – Composite Bonding
- Setting Up a Dental Surgery – Dental Equipment
- The Business of Veterinary Dentistry – Improving the Bottom Line
Introduction to Direct Pulp Capping (Partial Coronal Pulpectomy)
Endodontics is the branch of dentistry that deals with the prevention, diagnosis and treatment of conditions and injuries of the dental pulp and surrounding periapical tissues. Endodontic treatment, when compared with extraction, may be the quickest, easiest and least traumatic method of treating a tooth with pulpal disease. It enables the patient to maintain a full, healthy dentition, is more personally satisfying for the veterinarian and increases the number of services a practice may offer. Extraction, usually, is not the only solution, because the teeth of small animals respond very well to endodontic treatment.
Endodontic treatment may be required when the pulp is exposed to the oral cavity, is inflamed, is undergoing irreversible inflammation or is necrotic. Veterinary endodontics is concerned mainly with the treatment of infectious injuries due to fractured teeth, attrition, caries, canine odontoclastic resorptive lesions or anachoresis. The dental pulp may easily be injured by a concussive shock, such as a cricket bat or ball, or from continuous bone chewing or stick carrying. When the pulp is traumatised, it becomes inflamed (pulpitis) and swells (pulpal oedema) or haemorrhages (pulpal haemorrhage). If a fracture occurs exposing the pulp, it is bathed in saliva containing bacteria and becomes infected, leading to inflammatory pulpitis and oedema.

A recently fractured mandibular canine tooth demonstrating an exposed pulp canal and pulp tissue from a tiger at Taronga Zoo, Sydney.
Pulpal anatomy
The external tooth anatomy gives the veterinarian an approximate guide to the internal structure of the tooth. The internal space that the pulp occupies is termed the pulp cavity, which is then divided into the pulp chamber in the tooth crown and the root canal in the tooth root. The pulp is the mature form of the dental papilla. It can generally be assumed that a single pulp canal occupies each root, but occasionally more than one does exist. The pulp contains nerves, blood vessels, lymphatics, odontoblasts, fibroblasts, defense cells, and neurovascular tissues. In mature teeth of dogs and cats, at the apical constriction, there are many foramina (6-90 openings) entering each root canal, forming an apical delta.

Dye study of the apical delta of a dog’s canine tooth showing multiple foramina (Wiggs, Veterinary Dentistry).
At the apex of the tooth, the pulp becomes continuous with the periodontal ligament, and the neurovascular supply enters the pulp via the apical foramina.
Pulp tissue consists of four layers. The odontoblastic layer covers the periphery of the pulp cavity, with processes extending into the dentinal tubules. Weil’s basal layer (cell-poor layer), lies next to the odontoblastic layer. A cell-rich layer is located between the cell-poor layer and the fourth layer, which is the central pulp.
The tooth is formed in the mouth and as the tooth develops, i.e. crown and root development, dentine is produced by the odontoblasts (primary dentin). The odontoblasts lining the pulp then produce dentin throughout the life of the tooth (secondary dentin) and this results in thicker dentine walls and a narrower pulp cavity and canal.
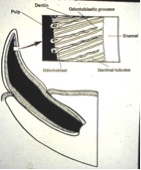
Diagram showing the root structure with odontoblastic processes within the dentinal tubules of an immature canine tooth (Wiggs, Veterinary Dentistry).
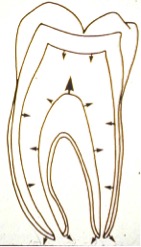
Schematic diagram of dentin formation in a mandibular molar with time. (Walton and Torabinejad, Principles and Practice of Endodontics)
Direct Pulp Capping (Partial Coronal Pulpectomy)
The pulp may be exposed following a traumatic injury that fractures the crown resulting in immediate pulp exposure. When the tooth is recently fractured and the pulp is exposed, the pulp at the site of exposure should appear healthy and haemorrhage on sterile probing. The tooth should be washed with copious amounts of sterile saline and haemostasis obtained following gentle pressure using a sterile pledget or a blunt ended absorbent paper point. Once haemostasis is achieved, a dressing of calcium hydroxide is placed, followed by a permanent restorative.
The clinical steps include:
- Usual pre-anaesthetic examination, general anaesthesia.
- Prior to the procedure the pet should be administered amoxicillin @ 20mg/kg IV (or an equivalent antibiotic).
- Examine tooth crown for any unstable pieces which are removed to obtain a completely solid crown.
- Place local nerve block.
- Radiograph to confirm intact and healthy root.
- Sterilise crown with chlorhexidine solution (such as Hexarinse).
- With a tapered diamond bur in water-cooled high speed handpiece perpendicular to crown remove any sharp enamel edges.
- Remove 5mm of coronal pulp from pulp cavity or canal using a sterile round diamond bur in water-cooled high-speed handpiece.
- Flush pulp with saline and place the blunt end of a sterile paper point over pulp stump and leave for five minutes. Haemostasis may be difficult to achieve in freshly fractured teeth, but can be obtained with gentle pressure using a sterile cotton pledget or blunt-ended absorbant paper point for a further five minutes. If the bleeding persists once the paper point is removed, remove a further 2mm of coronal pulp and pressure re-applied.
- Once haemostasis is achieved, place a one mm layer of calcium hydroxide powder, calcium hydroxide paste (LIFE or Biodentine) or MTA directly onto the pulp surface. The calcium hydroxide, which has an alkaline of 13, initiates necrosis of the pulp tissue and stimulates odontoblasts to produce tertiary dentin and therefore a dentin bridge over the healthy pulp.
- Remove any excess calcium hydroxide from the internal walls of your access hole and place a two mm layer of reinforced glass ionomer cement over the calcium hydroxide. Glass ionomer restorative performs two functions: 1. It forms a hermetic seal preventing ingress of oral bacteria into the pulp prior to the dentinal bridge forming, and 2. provides a firm base against which the composite restorative can be placed without disturbing the calcium hydroxide.
- Acid etch the glass ionomer, dentin and enamel with 37% phosphoric acid gel, rinse off after 30 sec, then dry thoroughly.
- Place a composite bond/adhesive.
- Place your composite restoration into the pulp canal or level of the fracture. Build up the composite in two mm increments.
- Finally, finish and smooth the composite and tooth with finishing burs.
- Then place another layer of light cured adhesive over this to seal any exposed dentinal tubules at the fracture or amputation site.
- Following the procedure, the pet should be administered antibiotics and pain control, which amoxicillin 10mg/kg BID PO, clindamycin 5.5mg/kg BID PO and a NSAID PO for 7 days should be sufficient.
- The pet should be fed soft food for 90 days and not chew bones, sticks or hard products, as well as, have their teeth brushed daily to decrease plaque accumulation. Brushing with Maxiguard or Hexarinse will aid in plaque control
- The tooth must be radiographed to confirm success. This is determined by the formation of a dentin bridge and narrowing of the pulp canal. The bridge will appear as a radio-opaque line above the pulp stump in 90 days post-procedure. The width of the pulp canal can be compared to the original radiograph taken at the time of the procedure.
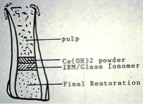
Diagram of treatment stages of the partial coronal pulpectomy.

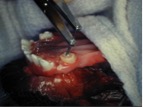
Pulp exposure and haemorrhage post fracture.
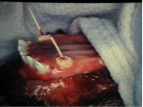
Placement of paper points into the canal, after pulp amputation of 5mm depth, in order to achieve haemostasis.
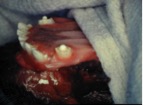
After achieving haemostasis, placement of calcium hydroxide over the pulp stump.

Note the white appearance of the calcium hydroxide in the pulp canal.
Placement of a hard setting glass ionomer restorative.

After removing excessive glass ionomer restorative, placement of acid to etch the dentine and enamel.

Using a blue wavelength curing light to cure “harden” the composite restorative material.

Using an explorer probe to confirm composite has cured, set hard, and there are no sharp edges to the tooth crown.